
1.
Malaria Basics
Malaria is an infectious parasitic disease. It's naturally transfered by a female mosquito of the kind anopheles from man to man. Another way of transfer can be by blood transfusion or other injections (with used syringes) with parasite - containing blood. Smallest amounts of blood already allow a transfer. Pregnant mothers can in certain cases transfer malaria to their child, but it's not necessarily so.

A poster warning before mosquitoes. Seen at a hospital in Chumpon, south Thailand. Image by Asienreisender, 2012
The development of the parasite happens exclusively inside anopheles mosquitoes and human bodies. There are three different kinds of malaria. Meaningful for travellers in Southeast Asia is malaria tropica, the most dangerous one. The others are malaria tertiana (which was widespread also in Europe, up to middle- and northern Europe until the first half of the 20th century) and malaria quartana.
Famous malaria patients of the European past were Albrecht Duerer, Oliver Cromwell and Friedrich Schiller. Malaria was finally extinct from Europe not before the 1960s due to the 'Global Malaria Eradiction Program' (see below).
The French explorer Henri Mouhot died 1861 near Luang Prabang in Laos due to malaria, and Alfred Russel Wallace concluded the mechanism of natural selection when he was shaken by malaria fevers in the Malay Archipelago.
A famous Asian malaria victim was Mohandas Gandhi (1869 - 1948), who suffered a severe attack in Aga Khan Palace in Pune in 1942, where he was held as a political prisoner.
All these three kinds of malaria are human-specific, means they don't infect animals (apart from very few exceptions at monkeys, some of them observed at macaques in Southeast Asia).
Anopheles mosquitoes are (together with aedes und culex mosquitoes) among the most widespread mosquito kinds. There are 360 different kinds of anopheles mosquitoes alone in the world, of whom 45 potentially carry malaria. Their habitats are not limited to the tropes and subtropes, but spread out until the borders of arctic regions.
Around 40% of the global human population lives in areas infested with malaria, of whom 300 - 500 million people are infected (according to the Robert Koch Institute, Berlin). More than 80% of them live in tropical Africa, 13.8% live in Asia.
In mountainous areas above 1.500m, near the equator from 2.500m on anopheles mosquitoes do not appear anymore. Malaria is pandemic in almost whole Southeast Asia. Indonesia and Burma / Myanmar have here by distance the most cases in percentage of the population. A growing resistance to antimalarials are a challenge in the Greater Mekong Sub-Region.
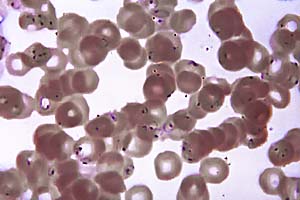
The exciter for malaria tropica is the parasite plasmodium falciparum, the most lethal one among the four plasmodium parasites. Estimated 1.8 million people died in 2004 worldwide, 1.2 million in 2010 due to malaria.
Let's assume that a biting mosquito is sucking blood. When the bitten human is malaria infected, the mosquito sucks with the blood the exciters which transfer within 8 to 16 days inside the mosquito into another phase and next to it's final stage. When it gets injected then into another humans blood circulation, reaching there the human liver, it's again breeding and spreading out into the vascular system. The perpetuation of the circle is then completed.
Read here more on the feeding habits of mosquitoes.